If you graduated from massage therapy school and immediately felt confident about your SOAP notes, you’re in the minority. For most new therapists, documentation is the part of the job that nobody quite prepares you for. You know the hands-on work. You understand anatomy. But translating a sixty-minute session into a clear, professional clinical record? That takes practice.
The good news is that SOAP notes don’t have to be complicated. Once you understand the framework and build a consistent habit, documentation becomes second nature. And it protects both you and your clients along the way.
This guide breaks down exactly what SOAP notes are, why they matter, and how to write them efficiently so you can spend less time on paperwork and more time doing the work you love.
What Are SOAP Notes?
SOAP is an acronym that stands for Subjective, Objective, Assessment, and Plan. It’s a standardized documentation method used across healthcare professions, including massage therapy, to record what happened during a client session in a structured, consistent format.
Each section of a SOAP note captures a different type of information:
- Subjective: What the client tells you. Their symptoms, concerns, pain levels, and goals for the session.
- Objective: What you observe and do. Your clinical findings, techniques applied, areas treated, and measurable observations.
- Assessment: Your professional evaluation of the client’s condition and how they responded to the treatment.
- Plan: What comes next. Recommendations for future sessions, homecare instructions, referrals, or follow-up timelines.
Think of it as a clinical narrative: the client’s story, your observations, your professional interpretation, and the path forward.
Why SOAP Notes Matter for Massage Therapists
It’s tempting to view documentation as busywork. Something you rush through between clients. But well-written SOAP notes serve several critical purposes that directly impact your career and your clients’ outcomes.
Legal Protection
Your SOAP notes are a legal record of the care you provided. If a client ever files a complaint or an insurance claim is disputed, your notes are the primary evidence of what happened during the session. Vague or incomplete notes leave you vulnerable. Detailed, consistent documentation protects you.
Continuity of Care
Clients don’t always see the same therapist, especially in multi-therapist clinics. SOAP notes ensure that any therapist picking up a returning client can quickly understand their history, what’s been tried, what’s working, and what to focus on. Without good notes, the client has to repeat themselves. And you’re starting from scratch every session.
Insurance and Third-Party Billing
If your practice bills insurance, motor vehicle accident claims, or workers’ compensation, proper SOAP documentation is required. Incomplete or poorly structured notes can result in denied claims and lost revenue, which is why having massage therapy client records organized and standardized is so important.
Professional Growth
Reviewing your own notes over time reveals patterns in your clinical reasoning. You’ll notice which techniques consistently produce results, which conditions you encounter most frequently, and where you might benefit from additional training. Documentation is a feedback loop for your own development.
How to Write Each Section of a SOAP Note
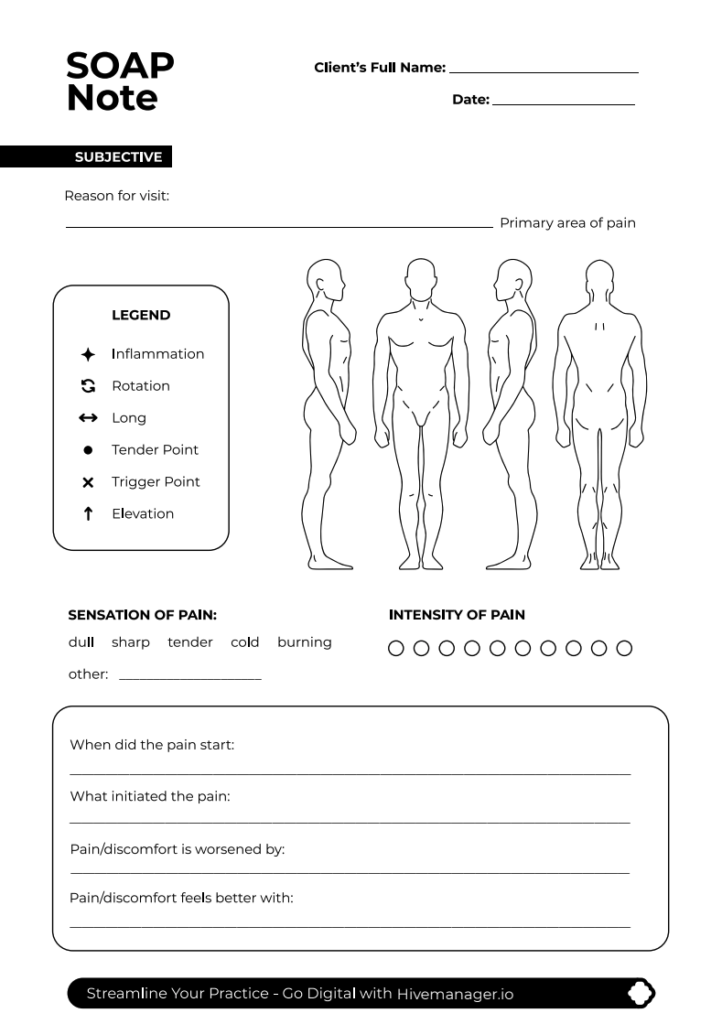
Let’s walk through each section with practical guidance and examples specific to massage therapy. If you prefer structure while you practice, you can also use a free SOAP notes template for massage therapists alongside this guide.
Subjective
This section captures the client’s own words and perspective. Record their chief complaint, location and severity of pain or discomfort (a numeric scale from one to ten works well), any changes since their last visit, relevant lifestyle factors like activity level, stress, or sleep quality, and their goals for the session.
For example: “Client reports persistent tightness in the right upper trapezius region, rating pain at six out of ten. States that the discomfort increases after prolonged desk work. Requests focus on the neck and shoulder area. Reports that stretching exercises from the last session provided temporary relief.”
Keep it factual. Document what the client tells you, not your interpretation of it. That part comes later.
Objective
This is where you record your clinical observations and the treatment you provided. Include postural or range-of-motion observations, areas treated and techniques used, duration of the session, tissue quality findings such as adhesions, hypertonicity, or trigger points, and any measurable outcomes like improved range of motion post-treatment.
For example: “Sixty-minute session. Observed forward head posture and elevated right shoulder. Applied deep tissue massage and myofascial release to the right upper trapezius, levator scapulae, and cervical paraspinals. Trigger point therapy applied to two active trigger points in the upper trapezius. Client’s cervical lateral flexion improved from approximately thirty degrees to approximately forty-five degrees post-treatment.”
Be specific with your language. Name the muscles. Note the techniques. Use measurable observations wherever possible.
Assessment
The assessment is your professional interpretation of the session. This is where you connect what the client reported with what you observed and treated. Note how the client responded to the treatment, whether symptoms improved, stayed the same, or worsened, your clinical impression of the condition, and any relevant patterns you’ve identified across sessions.
For example: “Client responded well to the deep tissue work and trigger point therapy. The hypertonicity in the right upper trapezius was noticeably reduced post-session. Improved cervical range of motion suggests muscular rather than structural limitation. The pattern of tension is consistent with prolonged static posture related to the client’s desk-based work.”
Plan
The plan outlines next steps. This section should include your recommended treatment frequency and next appointment, homecare instructions such as stretches, heat or ice application, or ergonomic adjustments, any referrals to other professionals if warranted, and goals for the next session.
For example: “Recommend follow-up session in seven to ten days with continued focus on the cervical and upper thoracic region. Homecare: gentle upper trapezius stretches twice daily, ergonomic workstation review recommended. Will reassess trigger point activity at the next visit.”

Common SOAP Note Mistakes to Avoid
New therapists tend to fall into a few predictable traps when they’re learning to document. Here are the most common ones and how to avoid them.
- Being too vague. “Worked on the back” tells you almost nothing. Which muscles? What techniques? What did you find? Specificity is what gives your notes clinical and legal value.
- Mixing subjective and objective information. Keep the client’s words in the subjective section and your observations in the objective section. If the client says their shoulder feels tight, that’s subjective. If you palpate hypertonicity in the upper trapezius, that’s objective.
- Skipping the assessment. Many new therapists just document what was said and what was done, then jump to the plan. The assessment is where your clinical reasoning lives. It’s what distinguishes a professional record from a basic session log.
- Writing notes hours or days later. The longer you wait, the less accurate your notes become. Aim to complete your SOAP notes within a few minutes of finishing each session while the details are still fresh.
- Using overly casual language. Your notes are a clinical and potentially legal document. Use professional terminology. Instead of “client said their neck was really sore,” write “client reports significant pain in the cervical region.”
Streamlining Your SOAP Notes with Technology
Handwritten notes on paper charts were standard for decades, but they come with real limitations. They’re hard to search, easy to lose, difficult to share between therapists, and time-consuming to maintain. As your client base grows, paper documentation quickly becomes a bottleneck.
Electronic charting software solves these problems by giving you structured templates, pre-populated fields, and the ability to access any client’s history in seconds. Dedicated tools for online SOAP notes and client charting are faster to write, easier to read, and far more secure than paper records stored in a filing cabinet.
Purpose-built platforms designed for massage therapy take this a step further. Instead of adapting a generic medical charting tool to fit your workflow, you get templates and fields that match how massage therapists actually document. The right terminology, the right structure, and all-in-one practice management tools with integration with the rest of your practice management tasks like scheduling, intake forms, and billing.
The efficiency gains are significant. Therapists who switch from paper to digital charting consistently report spending less time on documentation per client while producing more detailed, more consistent records. When charting is integrated with massage therapy scheduling and client management software, that means less admin time between sessions and better care over the long run.
Building the Documentation Habit
SOAP notes are one of those skills that feels burdensome at first but quickly becomes automatic with repetition. The key is consistency: use the same structure every time, write your notes immediately after each session, and review them periodically to refine your process.
Start simple. You don’t need to write a novel for every session. A concise, well-structured SOAP note that covers each section clearly is far more valuable than a lengthy, rambling one. As you gain experience, your notes will naturally become more nuanced and efficient, especially if you keep learning from massage therapy business tips and documentation tools.
Your documentation is a reflection of your professionalism. It protects your clients, protects your practice, and helps you grow as a clinician. Invest the time to get it right, and it will pay dividends throughout your career.
Ready to streamline your SOAP notes? Hivemanager’s electronic charting feature is built specifically for massage therapists, with structured SOAP note templates, integrated client records, and a workflow designed around how you actually practice. Start your free 14-day trial at hivemanager.io.